Ayurveda has a unique approach to diagnosis, which is holistic and based on observing the patient’s physical, mental, and emotional state. The main diagnostic methods in Ayurveda are collectively known as "Ashta Vidha Pariksha" (Eightfold Examination) and "Trividha Pariksha" (Threefold Examination).
Glaucoma
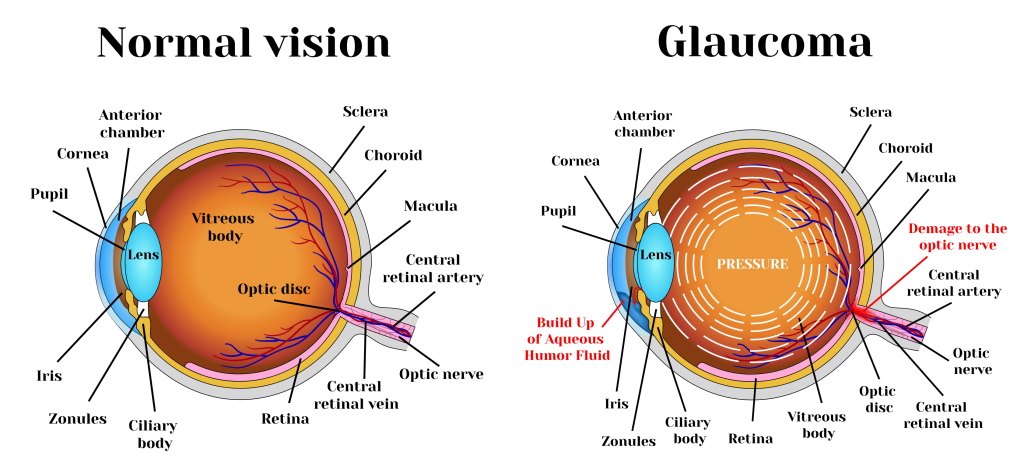
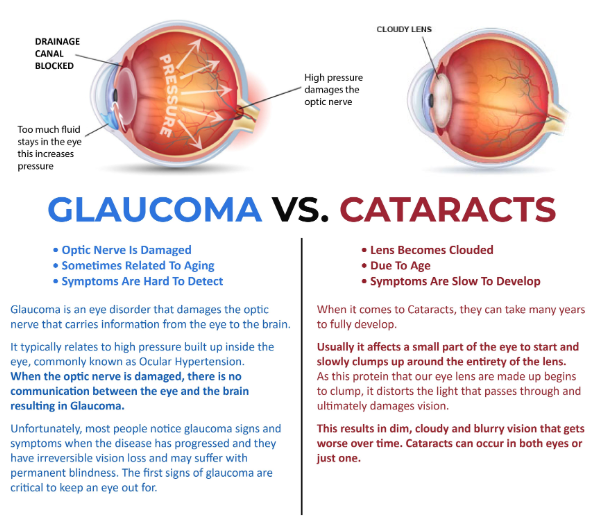
Glaucoma is a progressive optic neuropathy characterized by irreversible damage to the optic nerve due to elevated intraocular pressure (IOP), leading to gradual visual field loss. It is the second leading cause of blindness worldwide and is often asymptomatic in early stages.
II. Classification of Glaucoma
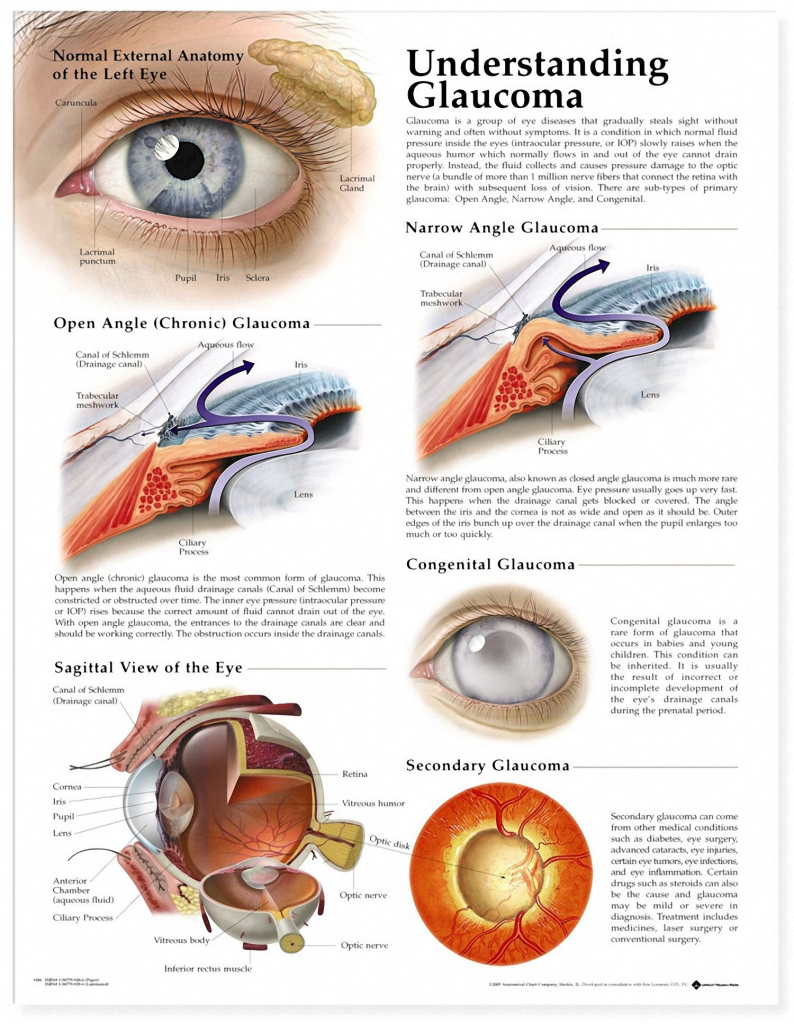
1. Primary Glaucoma (No identifiable cause)
Primary Open-Angle Glaucoma (POAG) – Most common type, slow progression
Primary Angle-Closure Glaucoma (PACG) – Sudden IOP rise, medical emergency
2. Secondary Glaucoma (Due to underlying pathology)
Neovascular Glaucoma – Associated with diabetes, retinal vein occlusion
Pseudoexfoliative Glaucoma – Deposition of material on lens & trabecular meshwork
Identifies early glaucomatous changes before visual field defects
4. Visual Field Testing (Perimetry)
Defect Type
Clinical Significance
Arcuate Scotoma
Early glaucoma
Nasal Step
Classic finding in POAG
Tunnel Vision
Advanced glaucoma
5. Pachymetry (Corneal Thickness)
Thin cornea (<500 µm) → Higher risk of glaucoma
6. Fundus Examination (Optic Nerve Head)
Cup-to-Disc Ratio (C:D) > 0.6 → Glaucoma suspicion
Vertical Notching of Disc → High specificity for POAG
VII. Management of Glaucoma
1. Medical Management (IOP Reduction)
Drug Class
Mechanism
Examples
Prostaglandin Analogs
↑ Aqueous outflow
Latanoprost, Bimatoprost
Beta-Blockers
↓ Aqueous production
Timolol, Betaxolol
Alpha-Agonists
↓ Aqueous production & ↑ Outflow
Brimonidine, Apraclonidine
Carbonic Anhydrase Inhibitors
↓ Aqueous production
Acetazolamide, Dorzolamide
Miotics (Cholinergics)
↑ Trabecular outflow
Pilocarpine
2. Laser Procedures
Procedure
Indication
Laser Trabeculoplasty (ALT/SLT)
POAG, increases outflow
Laser Peripheral Iridotomy (LPI)
Angle-closure glaucoma
Cyclophotocoagulation
Refractory glaucoma
3. Surgical Management
Surgery
Indication
Trabeculectomy
Moderate-severe glaucoma
Tube Shunt Surgery
Refractory glaucoma
Minimally Invasive Glaucoma Surgery (MIGS)
Early-stage glaucoma
VIII. Glaucoma Progression Monitoring
✅ IOP Monitoring – Target IOP depends on severity ✅ Visual Field Testing – Every 6 months ✅ OCT/RNFL Analysis – Detects progression before field loss
IX. Summary & Key Takeaways
✅ Glaucoma is an irreversible optic neuropathy with gradual vision loss. ✅ Elevated IOP is a major risk factor but not always present. ✅ OCT & visual field testing are critical for early diagnosis. ✅ Prostaglandin analogs are first-line medical treatment. ✅ Laser & surgical options are used for refractory cases.